About two years ago we reported on a remarkable piece of research showing that pigeons were pretty good at picking out diseased from normal tissue samples presented to them as either stained sections or X-ray images (Intelligence: Of Birds, Men and Machines). Making this selection is currently a huge challenge for pathologists and radiologists. So the notion that, if the machine that is a bird’s brain is so smart, maybe we can apply machine learning — the branch of artificial intelligence (AI) and computer science which models data to imitate the way that humans learn, gradually improving its accuracy.
Expanding AI
In the November 2021 piece we summarised how AI was already being applied to every medical imaging method — MRI, CT, ultrasound and X-ray — and to major cancers, notably lung through, in particular, the UK TRACERx studies that we caught up with in the two previous blogs (Little Things … & A Moving Picture). We also reviewed the TOAD method for identifying the origin of primary tumours and how the DenSeeMammo software had reached the point of matching the performance of radiologists in predicting breast cancer risk from mammograms.
Rapid progress
The intervening two years have seen progress to the extent that Kristina Lång and her colleagues at Lund University in Sweden have now shown that AI screening is as good as two radiologists working together and almost halves the workload. This was the first randomised controlled trial of its kind and it involved more than 80,000 women. The novel approach was to compare AI-supported screening directly with normal screening by having half the scans assessed by two radiologists and assessing the other half by AI-supported screening followed by interpretation by one or two radiologists.
The critical result was that 244 women (28%) recalled from AI-supported screening were found to have cancer compared with 203 women (25%) recalled from standard screening. That is, 41 more cancers were detected using AI, of which 19 were invasive and 22 were in situ cancers.
Importantly, using AI did not generate more false positives (an incorrect diagnosis of a scan as abnormal) — the false-positive rate was 1.5% in both groups.
But only one step
This latest work will be greeted with huge relief — not only among radiologists who can look forward to some of the pressure being lifted from their shoulders but also in the wider medical community as advances in the use of AI make it an ever more valuable tool.
About six years ago an eye-catching paper appeared showing that pigeons were remarkably good at identifying disease in humans on the basis of stained tissues presented on microscope slides or medical images (e.g., X-rays). In other words they could make a pretty good fist of the task that confronts pathologists and radiologists on a daily basis — and immense the task is if you think about the number of tissue samples that are assessed every day around the world and of the consequences that might follow an incorrect classification.
The evidence that pigeons might be quite good at this sort of pattern recognition came from Richard Levenson and colleagues from the University of California, the University of Iowa and Emory University. The idea was, in principle, simple: confront the birds with images and teach them to tap the correct colour band by giving them food when they got it right – i.e. distinguished diseased from normal samples.
Bird brain’s office. The pigeons’ chamber has a food pellet dispenser and a touch-sensitive screen. The medical image (centre) is flanked by choice buttons (blue and yellow rectangles for benign or malignant sample) activated by pecking. From Levenson et al., 2015.
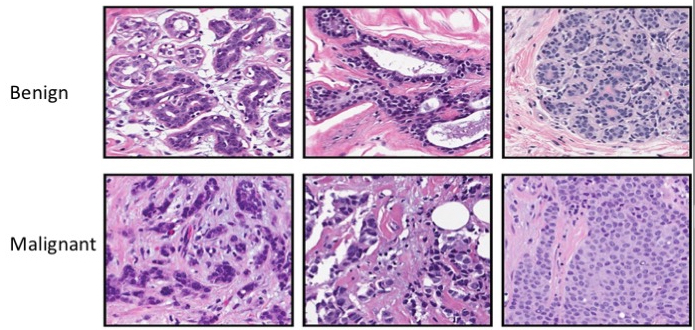
Benign versus malignant. The images are slices of breast tumours stained with a dye. Top row: benign; Bottom row: malignant. Confronted with these pictures pigeons first performed with chance levels of accuracy but they quickly learned to discriminate. From Levenson et al., 2015.
The images above illustrate the challenge faced by pathologists. Radiologists attempting to decipher X-ray and CT images face similar difficulties. Astonishingly, Levenson et al. were able to train pigeons to a high standard of discrimination. It remains unlikely that white-coated avians will be seen any time soon fluttering along the corridors of our hospitals but it does raise the notion that, if pigeons are so smart, maybe we can harness artificial intelligence to help with the problem of screening tissues.
The science of artificial intelligence began in 1956 and in Taking Aim at Cancer’s Heartwe described the saga that led to an IBM computer beating the then world chess champion — an example of machine learning whereby a sequence of instructions (an algorithm) defined the patterns that could be formed by the pieces on the chequerboard, enabling a computer to outpace the human brain. In that blog we described the application of pattern recognition to mutations in cancer that enabled future genetic changes to be predicted and hence how cancers will evolve.
Applying artificial intelligence …
Much commercial effort is now going into automated, artificial intelligence-based, ‘smart workflows’ to support radiographers in the use of every major imaging modality – MR, CT, ultrasound and X-ray. These too use machine learning — a set of instructions that focusses on recognizing data patterns. Training data sets comprise examples denoted as ‘cancer’ or ‘not cancer’. When presented with a new image the algorithm works out which group it falls into.
To lung cancer
A number of AI projects are focussed on lung cancer because its early symptoms are often ignored and by the time it is diagnosed treatments are relatively ineffective. However, there’s also a practical reason in that lung tumours have a much greater difference in radio density relative to air than any other organ. The technique of X-ray computed tomography (CT) was developed by Sir Godfrey Hounsfield and Allan Cormack and the Hounsfield Unit (HU) is a quantitative scale for measuring radiodensity. The figure for air is about 1000 HU: for a solid lung tumour lump the range is 20-100 HU.
Diego Ardila and colleagues at Google AI, Mountain View, California trained their system using a database of more than 40,000 CT scans (Ardila et al. 2019). These included both patients with lung cancer and individuals who had not been diagnosed with the disease. They instructed the computer which early-stage scans turned out to contain cancerous spots and which did not. With time the computer gradually improved in being able to discern malignant spots from benign ones. Eventually their system correctly identified the early stages of lung cancer 94% of the time and out-performed a group of experienced radiologists.
In the UK the TRACERx (TRAcking Cancer Evolution through therapy (Rx)) lung study is a nine-year, multi-million pound research project run by the Institute of Cancer Research, London. A key aim is to look at what is going on within the tumour (intratumour heterogeneity) and how that relates to clinical outcome. It’s also examining the impact of treatment regimens. Khalid AbdulJabbar, Charles Swanton, Yinyin Yuan and colleagues recently reported that, after training the computer on hundreds of images of early stage lung tumours, the system acquired the capacity to select tumours with regions low in immune cells. It emerged that these are more likely to relapse after surgery to remove tumour tissue or drug treatment (chemotherapy). The capacity to acquire this sort of information in the early stages of lung cancer has important implications for treatment and in particular for guiding immunotherapy.
To breast cancer
DenSeeMammo is a fully automated software system design to tackle the problem of breast density in mammography screening. The density of breast tissue is variable — it’s dense if there’s a lot of fibrous or glandular tissue and not much fat — and it poses a problem in detecting abnormal growths. Fiona Gilbert, Olivera Djuric and colleagues from the University of Cambridge and a number of other European institutes have now developed this platform to the point where it can equal the performance of radiologists in predicting breast cancer risk. They showed this in an analysis of more than 14,000 2D mammograms from several European studies. Even more excitingly, this automated system performed even better in predicting interval cancers (these are cancers diagnosed after a negative mammogram but before the next mammogram screen). These results suggest that DenSeeMammo and ongoing improvements in automated screening will become a significant aid to radiologists in assessing mammographic images.
To cancers of unknown origin
Other recent studies show how this field is progressing across the spectrum of cancer diagnosis. Ming Lu, Faisal Mahmood and colleagues at Harvard devised the appealingly named TOAD (Tumour Origin Assessment via Deep Learning), a deep-learning-based algorithm that could identify the origin of primary tumours. This is important because knowing the site of a primary tumour is important in guiding the treatment of metastatic tumours and, despite advances in tissue testing, about 2% of cancers cannot be categorised in terms of their origin.
Much like the pigeon studies, they used whole-slide images of tumours with known primary origins to ‘train’ a computer model to distinguish primary from metastatic tumours and to predicts sites of origin. The basic idea is to segment the area of the slide into tens of thousands of regions — small patches. Computers digitize the information for analysis — it’s virtual microscopy and the method is now called digital pathology.
The performance of a machine learning model can be checked using an ROC (Receiver Operator Characteristic) curve and measuring the area under the curve (AUC). In general, an AUC of 0.5 suggests no discrimination, 0.7 to 0.8 is considered acceptable, 0.8 to 0.9 is considered excellent, and more than 0.9 is considered outstanding. For distinguishing primary from metastatic tumours TOAD achieved AUC-ROC values greater than 0.95. Similar levels of performance were obtained in identifying sites of origin.
It’s worth emphasising that in the analysis of tissues the idea is not that computers will replace humans but that they will become able to sort samples in to positive, negative and unresolved. The enormously valuable upshot will be that expert human eyes can focus on the tricky ones and be spared the strain of dealing with those that are clear-cut.
Based on genomic profiles P-NET can predict the potential for recurrence and identify molecular drivers — i.e. critical mutations. As with TOAD, P-NET requires tuning and training before use. Specifically Elmarakeby’s group rediscovered known genes implicated in prostate cancer (AR (androgen receptor), PTEN, TP53 and RB1) but they also found novel candidate genes, e.g., MDM4 and FGFR1, implicated in advanced disease. MDM4 inhibits p53 and FGFR1 (Fibroblast Growth Factor Receptor 1) can promote tumour progression and metastasis. Their results suggest that MDM4-selective inhibitors may be effective in metastatic prostate cancers that retain a normal TP53 gene.
Thus, in addition to pattern recognition, methods based on machine-learning for the analysis of tumour DNA sequences can reveal both specific mutations and biological pathways, providing a powerful insight into the processes involved in cancer progression and guidance in translating these discoveries into therapeutic opportunities.
Giorgi Rossi P, Djuric O, Hélin V, et al. (2021). Validation of a new fully automated software for 2D digital mammographic breast density evaluation in predicting breast cancer risk. Sci Rep. 2021;11(1):19884. doi:10.1038/s41598-021-99433-3.